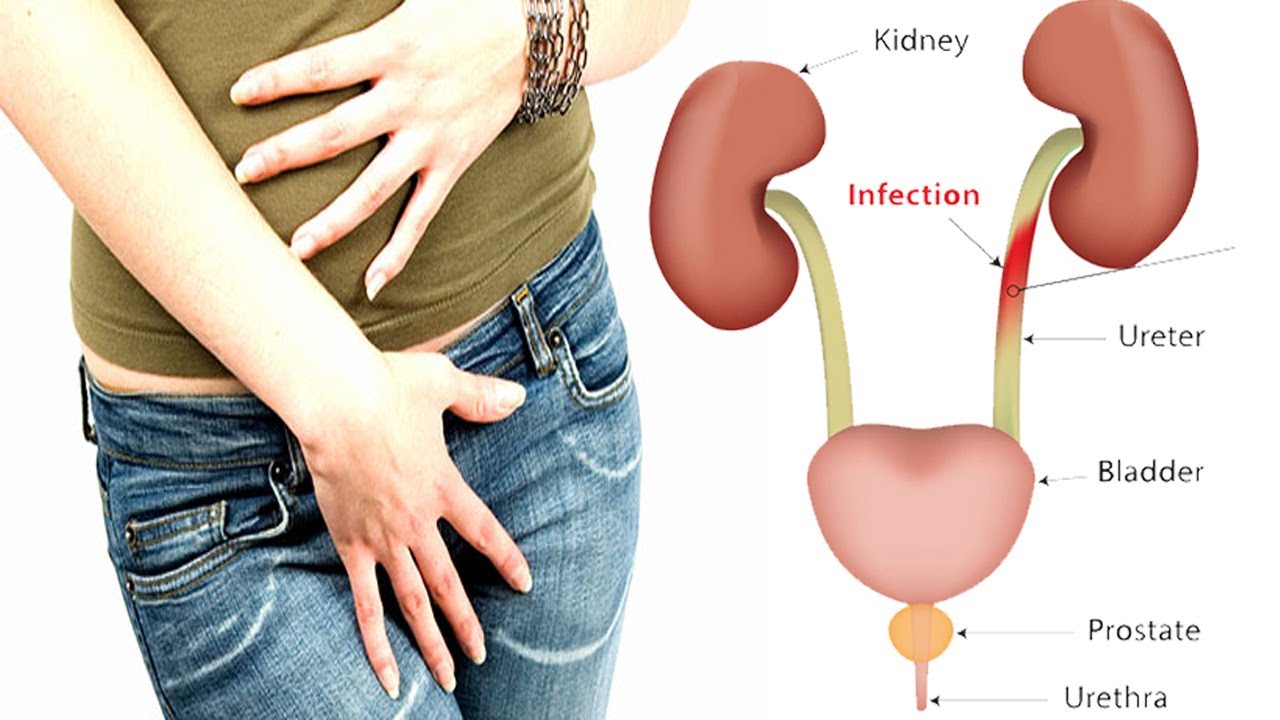
Transmission and Pathogens. Catheter-related urinary tract infection (UTI) occurs because urethral catheters inoculate organisms into the bladder and promote colonization by providing a surface for bacterial adhesion and causing mucosal irritation. The presence of a urinary catheter is the most important risk factor for bacteriuria.
Once a catheter is placed, the daily incidence of bacteriuria is 3-10%. Between 10% and 30% of patients who undergo short-term catheterization (ie, 2-4 days) develop bacteriuria and are asymptomatic. Between 90% and 100% of patients who undergo long-term catheterization develop bacteriuria. About 80% of nosocomial UTIs are related to urethral catheterization; only 5-10% are related to genitourinary manipulation.
The presence of potentially pathogenic bacteria and an indwelling catheter predisposes to the development of a nosocomial UTI. The bacteria may gain entry into the bladder during insertion of the catheter, during manipulation of the catheter or drainage system, around the catheter, and after removal.
Enteric pathogens (eg, Escherichiacoli) are most commonly responsible, but Pseudomonas species, Enterococcus species, Staphylococcus aureus, coagulase-negative staphylococci, Enterobacter species, and yeast also are known to cause infection. Proteus and Pseudomonas species are the organisms most commonly associated with biofilm growth on catheters.
Candida, especially Candida albicans, is the second-most-common organism that can cause catheter-associated urinary tract infection or asymptomatic colonization.
Risk factors for bacteriuria in patients who are catheterized include longer duration of catheterization, colonization of the drainage bag, diarrhea, diabetes, absence of antibiotics, female gender, renal insufficiency, errors in catheter care, catheterization late in the hospital course, and immunocompromised or debilitated states.
Guidelines for Catheter Use. The 2009 Centers for Disease Control and Prevention (CDC) guidelines for prevention of catheter-associated urinary tract infections (UTIs) recommends catheter use only for appropriate indications. Catheter use and duration should be minimized in all patients, especially those at higher risk for catheter-associated UTI (eg, women, elderly persons, and patients with impaired immunity).
Long-term catheterization increases patient satisfaction but also increases mechanical complications. Contraindications include bleeding disorders, previous lower abdominal surgery or irradiation, and morbid obesity. Intermittent catheterization is an option, but most patients become bacteriuric within a few weeks; the incidence of bacteriuria is 1-3% per insertion.
Diagnosis. Symptoms of catheter-related urinary tract infection (UTI) generally are nonspecific; most patients present with fever and leukocytosis. Significant pyuria is generally represented by more than 50 white blood cells (WBCs) per high-power field (HPF). Colony counts on a urine culture range from 100-10,000/mL.
Infections may be polymicrobial. Pyuria and elevated bacterial colony counts are seen in all patients in whom a catheter has been in place for more than a few days. In this situation, their presence is not synonymous with a UTI.
The 2009 Infectious Diseases Society of America (IDSA) guidelines define catheter-related UTI in patients whose urinary (urethral, suprapubic, or condom) catheter has been removed within the previous 48 hours by the presence of symptoms or signs compatible with UTI with no other identified source of infection along with 1000 or more colony-forming units (CFU)/mL of 1 or more bacterial species.
Treatment & Management. In some patients with bacteriuria, removal of the catheter suffices. To reduce the risk of urinary tract infection (UTI), antibiotic treatment may be considered in patients with asymptomatic bacteriuria that persists 48 hours after removal of a short-term indwelling catheter. A specimen for urine culture should be obtained before initiation of antibiotic therapy, because of the wide spectrum of potential infecting organisms and the increased likelihood of antimicrobial resistance.
In patients whose symptoms resolve promptly, 7 days is the recommended duration of antibiotic treatment. In those with a delayed response or with bacteremia, 10-14 days of treatment is recommended. In patients who are not severely ill, a 5-day regimen of a quinolone may be considered. In women older than 65 years who develop a UTI after removal of an indwelling catheter and who have no upper urinary tract symptoms, a 3-day antimicrobial regimen may be considered.
Prevention. Aseptic indwelling catheter insertion, a properly maintained closed-drainage system (with ports in the distal catheter for needle aspiration of urine), and unobstructed urine flow are essential for prevention of UTI. Because many of these infections occur in clusters, good hand washing before and after catheter care is essential.
Systemic antimicrobial drug therapy has repeatedly been shown to lower the risk of UTI in catheterized patients; the greatest benefit was observed in those catheterized for 3-14 days. Most hospitalized patients already are receiving antibiotics for other reasons. Disadvantages include creating resistant organisms.

.png)