The term healthcare-associated pneumonia (HCAP) was defined as pneumonia in nonhospitalized patients who had significant experience with the healthcare system. Such contact could include (1) intravenous therapy for wound care within the preceding 30 days, (2) residence in a long-term care facility, (3) hospitalization in an acute-care hospital within the preceding 90 days, and/or (4) outpatient treatment in a hospital or hemodialysis clinic within the preceding 30 days.
Pneumonia is defined as "new lung infiltrates plus clinical evidence that the infiltrate is of an infectious origin, which include the new onset of fever, purulent sputum, leukocytosis, and decline in oxygenation." Hospital-acquired pneumonia (HAP), or nosocomial pneumonia, is a lower respiratory infection that was not incubating at the time of hospital admission and that presents clinically 2 or more days after hospitalization.
HAP is a common nosocomial bacterial infection and is most prevalent in medical and surgical intensive care units (ICUs). As such, HAP adds significantly to the cost of hospital care and to the length of hospital stays. Patients with HAP develop fever and leukocytosis. These findings are a requisite for its presumptive diagnosis. Respiratory tract symptoms include an increase in respiratory rate and shortness of breath.
Inhalation, aspiration, and hematogenous spread are the 3 main mechanisms by which bacteria reach the lungs. The primary route by which organisms enter the lower airways is aspiration of oropharyngeal secretions into the trachea.
Primary inhalation pneumonia develops when these organisms bypass normal respiratory defense mechanisms or when the patient inhales aerobic gram-negative organisms that colonize the upper respiratory tract or respiratory support equipment.
Aspiration pneumonia is due to the aspiration of colonized upper respiratory tract secretions.
The stomach appears to be an important reservoir of gram-negative bacilli that can ascend and colonize the respiratory tract. A prospective observational study found that patients who used acid-suppressive medications were more likely to develop hospital-acquired pneumonia (HAP) than were patients who did not (5% vs 2%). The risk for pneumonia was significantly increased with proton pump inhibitors, but not with histamine 2–blocking agents.
Hematogenously acquired infections originate from a distant source and reach the lungs via the bloodstream.
The development of hospital-acquired pneumonia (HAP) represents an imbalance between normal host defenses and the ability of microorganisms to colonize and then invade the lower respiratory tract.
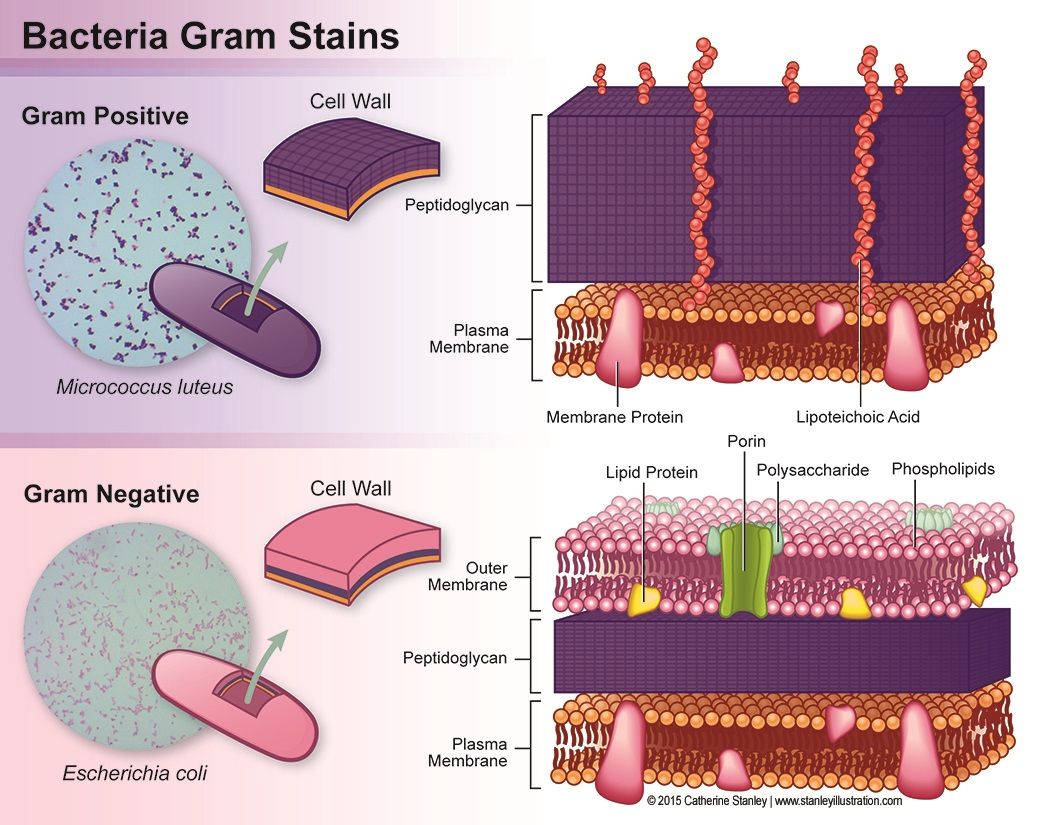
Because aerobic gram-negative bacilli (eg, Pseudomonas aeruginosa) are the major pathogens associated with HAP, the pathophysiology of nosocomial pneumonia relates to the destructive effect on lung tissue. Aerobic gram-negative pathogens may be divided into 2 categories. The first category includes organisms that cause necrotizing pneumonia with rapid cavitation, microabscess formation, blood-vessel invasion, and hemorrhage (eg, P aeruginosa). Alternatively, other nonnecrotizing gram-negative bacilli (eg, Serratia marcescens) may be responsible for nosocomial pneumonia.
Common bacteria involved in hospital-acquired pneumonia (HAP) include the following:
Differential Diagnoses of Nosocomial Pneumonia
All patients with presumed nosocomial pneumonia should undergo testing to rule out conditions that mimic nosocomial pneumonia. The diagnosis of nosocomial pneumonia is difficult because it may present in a very nonspecific fashion. A summary of management strategies is available through a recently released practice guideline provided by the Infectious Diseases Society of America (IDSA) and American Thoracic Society (ATS).
The wide list of differential diagnoses presents a major challenge in diagnosing nosocomial pneumonia. Many conditions other than nosocomial pneumonia mimic pulmonary infiltrates (eg, fluid, atelectasis) on chest radiographs.
Any disorder that results in leukocytosis with variable degrees of left shift may be included in the differential diagnoses. Noninfectious inflammation may produce fever.
Consider all of these differential diagnoses carefully before settling on a diagnosis and embarking on a course of antimicrobial therapy.
The most common causes of infiltrates in ventilated patients with fever and/or leukocytosis include the following conditions:
Microbiologic approach to diagnosing hospital-acquired pneumonia. If at all possible, patients should not be treated empirically. Antibiotic choice should be based on culture of sputum that is noninvasively obtained—spontaneously or by induction of sputum via nasotracheal suctioning or endotracheal aspiration in a patient who has been intubated because of HAP.
Serial chest radiography is most useful in ruling out progression of the pneumonia and serves as an indicator of the efficacy of appropriate antimicrobial therapy.